We spoke to a Doctor about his experience diagnosing and treating patients with Chronic Conditions.
You can watch the full interview above or read the transcript below. Jesse. Hey, I’m Jesse from Bearable welcome to the bearable podcast where we talk to medical professionals about the experiences of people with hard to diagnose conditions, chronic conditions, and hidden illnesses I hope you enjoyed this episode. All right, so welcome to the first episode of the bearable podcast. Today we’re joined by Dr Johannes Driessen. He is – full disclosure, my brother as well – a convenient guest for the first episode. We’re going to be talking to him today about his experience with patients who self-diagnose and also generally treating patients with hard to diagnose conditions as well. So Johannes do you want to give yourself a quick introduction and let our audience know how you became a Doctor? Dr Johannes. Yeah I mean you’ve mentioned the two most important things already; that I’m your brother and that I’m a doctor. So, yeah I’ve been a doctor for I think four four-ish years now so it’s something I started relatively later on in life and for the last couple of years I’ve been a GP trainee. So that’s a three or four-year process where we rotate three different hospital jobs and ultimately go into full-time GP training [which is] what I’ll be doing there in September. So, yeah it’s been a slightly non-traditional version of the training program but here I am working in south London. Living the dream… Jesse. Absolutely. Do you want to touch on anything you were doing before you went down this career path because you’ve had some kind of like I suppose relevant experiences prior to becoming a doctor as well right? In terms of maybe like the pharmaceutical work you did or even your first master’s degree? Dr Johannes. Yeah, it’s been a bit of a scattergun CV. So I did an undergraduate masters in neuroscience and as you mentioned I’ve kind of done a lot of part-time work in a pharmacy. So I was a dispenser part-time for about 15 years. I got a lot of kind of initial patient interaction over the counter in that way and I’ve done a couple of years in the defence industry in the military which is a bit of a segue away from healthcare and kind of physical sciences. Then headed back into medicine as my current and hopefully ongoing career. Jesse. Who knows with you. It could change at any moment. Dr Johannes. Yeah absolutely Jesse. I wondered as well if any of those past experiences, past educational [routes] or career paths have influenced or had an impact on your approach to being a doctor as well? Dr Johannes. Yeah it’s not something I’ve really reflected on that much. I think you know working in pharmacy gave me a lot of experience dealing with people and dealing with their kind of health anxieties. Sometimes having to kind of rationalize those anxieties a little bit. You know just from the perspective of someone who didn’t really have any qualifications but you know was giving health advice over the counter. I think the other thing is just having worked in kind of really different sectors of work so you know working in the military, working in healthcare and working for private companies you just meet a huge range of different people and personality types and you meet people with all kinds of different life views and world views. So I think it’s been good just to kind of see a much broader cross-section of the population that I now work with because I think if you start in one field and kind of stay there you can kind of see the world as a kind of bubble around you. So I guess that yeah that has been useful in just understanding human beings a little bit better. Jesse. That sounds like quite a useful skill to have if you’re going to be a doctor working with human beings every day. Dr Johannes. Absolutely you should all have 10 different careers and join the military for a few years before you try and understand people.How are doctors trained to handle patients with chronic conditions?
Jesse. I guess one of the things I’m interested in talking about first is the fact that you’re obviously still training. So I did want to ask you about how training maybe prepares you for people with how to diagnose conditions, chronic conditions, hidden illnesses. However, you [want to] refer to them. Is that something that there is explicit training for? Dr Johannes. I think it’s something which people are starting to address in medical education. I think it’s becoming something that universities are becoming more aware of and I think the whole way that medicine is taught is trying to move away from this kind of traditional paternalistic structure and understand medicine as more of a social construct. Trying to kind of adopt patient-centred care as opposed to doctor-centred care. But I think it’s still in its infancy and it’s something that people are still exploring and trying to fit into the existing structures of education and practice so I think at the university level it’s something that is just beginning to kind of happen in a real way. During my foundation training, which is the first two years of being a doctor, we had some really useful insights from some of the psychiatrists who help the medical and surgical doctors to find strategies for care. For these people, particularly in hospital settings, and to try and give an understanding of you know what some of these people and these patients with complicated medical conditions and what they’re experiencing and how we can work with them to try help them because quite often there isn’t a concrete solution to fixing these problems. Which is what a lot of people are looking for and what a lot a lot of doctors instinctively want to do. So it kind of to some extent it does kind of blow our minds because we’re taught about you know the body as a complex machine and when something doesn’t fit that stereotype it’s not that we don’t want to fix it or can’t fix it but it’s just a whole different mindset so we yeah we had some really really insightful input from one psychiatrist in particular but it is kind of it’s it’s a little bit of bonus material on top of a curriculum which isn’t really kind of skewed in that direction. Because although it’s becoming much more recognized it is still a relative minority group of conditions. So I think it’s something that is being recognized slowly and I think doctors are really grateful for being given those insights but it’s not something which is kind of a core part of the curriculum as I’ve experienced it so far. Jesse. I mean it’s reassuring in the first place that it is something that’s maybe increasingly being looked at. We’ll probably touch on this more [later], one of the problems is maybe that both patients and doctors are given a very short window in which to obtain a diagnosis. I think a lot of people who self-diagnose feel like they know what they have. They go to a GP appointment. There’s 10 minutes for them to try and convince the GP that they have this thing they think they have and it’s maybe not that simple. I guess a natural follow-up to that is; what is your real-world experience with people who have hard to diagnose conditions or come to you with a chronic condition? Do you have experience with patients like that? Dr Johannes. Yeah, so we’ve kind of we’ve talked in the past about how you know because I’m in training because I’m moving through different specialities at the moment, it’s not a type of patient that I work with regularly at the moment. But certainly, in the past, I’ve worked with patients who have yet one of a variety of complex medical conditions. Some people have certainly come in and told me for example that they have post-traumatic stress disorder when they haven’t kind of been assigned that diagnosis by a medical professional. They’re kind of confident that that’s the situation they’re in and similarly when I worked as a foundation doctor elsewhere there was a fairly substantial group of young women who had kind of chronic abdominal pain that would come into the physiological ward for diagnostic management of their conditions. So it’s something I have come across. I think for a lot of doctors it’s something that we kind of experience to some extent and I think when I’m working full time as a GP it’s something that I will experience a lot more, but each of those cases is really different and unique because everyone is different. There are similarities between the cases and I think one of the main similarities is that quite often you get this adversarial relationship between patients and doctors and that happens for a lot of reasons. Like you mentioned some people will either – through reading online or through forming communities with people who have similar symptoms and similar experiences – will kind of pick out a diagnosis that they feel is appropriate for them. Then going to the GP. You know these days you’ll quite often see a different GP every time because of the way that surgeries are set up [in the UK through the NHS] these days. You’ll kind of present your opening statement to a GP who has their own mental model of how to have a consultation with a patient which involves kind of delving into the background and trying to understand you and build some rapport and I think when you have the clash of the two mental models where the patient just wants to say “i have this condition what can you do for me” and the doctor has their own way of trying to draw out all of these clues about what’s going on, what’s happening. AND then if you combine that with the fact that there’s a huge amount of time-pressure to deal with. I think, quite often, that is an unsatisfactory consultation. And I think the more often that happens the more fraught both sides become and the more that a doctor might start to see a patient or a group of patients as being frustrating because they’re not playing by the doctor’s rules of how to help someone. Equally the patients kind of sat there thinking “oh it’s this person’s job to help me manage my condition and they’re just kind of wasting time asking me all these irrelevant questions either doing or not doing tests that I feel are relevant or are irrelevant or suggesting strategies which I don’t feel will help me”. Again, something that we’ve talked about before, is just how I think doctors and patients both need to have a lot more empathy and patience and open-mindedness about the fact that we’re not primarily trained to work with patients who have complex or difficult to define problems. And I think we both [patients and doctors] need to just be a bit more patient, a bit more understanding about the complexity of the health service in general. The limitations of the health service and if we both believe that we’re aiming for the same thing, which is to help each other to come to a kind of mutually beneficial understanding and to help the patients. I think we are much more likely to reach a satisfactory outcome for everyone. It’s a really difficult situation for both parties and I think really disheartening thing is when doctors kind of see these patients, there’s this kind of term; “heart-sync-patient” when someone comes into the room you know that their situation is complicated their life is complicated they’re probably not going to be able to help them the way they want. But it’s really derogatory to see a patient as a stressful, disappointing thing before they’ve even had that interaction with you. Equally, it’s really frustrating as a doctor when you are trying to help someone in your own way and they’re not allowing you to do your job in the way that you know how to do it.Why is it hard to diagnose a chronic condition in a 10-minute appointment?
Jesse. It sounds difficult. I think actually it’s maybe the reason behind why I wanted to have this conversation is that my personal experience has been – I think similar to a lot of the people that use bearable – which is that when I was in my early 20s I had an eating disorder, I had anorexia. I classified it that way myself, I’d self-diagnosed it as being anorexia because it ticked all of the boxes I associated with that illness. When I went to see my GP they essentially said to me “you don’t have that” or “I’m not going to treat you as though you have that” and I think I left feeling frustrated because it was something I’d lived with for over a year at that point and my expectation was like; I know I have this, I want this person to validate this. So can you actually explain from the doctor’s perspective why something like that is harder to diagnose or what the process might be to diagnose something that’s difficult? Why can’t it be done within 10 minutes? Why does it need to take longer? Dr Johannes. I can’t speak for the doctor that you had that interaction with and I think it’s really sad that you were kind of blocked so kind of abruptly in reaching a diagnosis. But yeah it again like everything we’re going to talk about today it’s complicated. I think to some extent – and something you’ve mentioned to me before – is that part of it will be to do with stereotypes and you know, we as medical students are taught about the stereotyped patient that might come in with a particular problem. So when a doctor or any member of the public imagines a patient with anorexia you’re probably not typical of that patient [being male] and certainly for a doctor who works with people with eating disorders they’re going to have a much more broad understanding of what a patient looks like who has anorexia and the trick is that you know that’s the tricky thing that that’s not the person you’re going to see first. You’re going to see someone who is much more of a generalist whether that’s your GP or someone else, it’s about working around the stereotypes that exist about all kinds of different conditions. So I think to some extent there will be a degree of, whether it’s subconscious or conscious bias, there will be issues about not fitting a stereotype of what a doctor is expecting to see in a person who has a condition. But equally, I think one of the things that get really tricky is the fact that all of these diagnoses, in general, are associated with a number of really specific criteria. So some diagnoses will be a diagnosis of exclusion where you kind of look for in 101 different things and if you can’t find any and you’re still left with this constellation of symptoms then you might say okay well “we’ve excluded all of these other things that must be this diagnosis” but for the majority of conditions – and especially conditions where there is a mental health dimension to them – there will be very specific criteria that you have to meet in order to receive a specific diagnosis. I think that’s not something that is very well understood by people who are experiencing these symptoms because you can have 99.9 per cent of the experiences in common with someone who has a diagnosis of anorexia – for example – but if you don’t meet the specific criteria that might just not be the name that we give it. There might be a subtly different name that you’re not familiar with which doesn’t feel right to you but it doesn’t necessarily mean that you’re being dismissed or that we’re not taking the condition seriously. I mean, obviously, there will be some cases where a doctor just thinks that maybe you don’t have the thing you think you have and that does happen sometimes. That people [doctors] do get caught up on a diagnosis that maybe doesn’t explain or would explain some of their symptoms but maybe you’re kind of looking in in the wrong direction for the answers and I think as human beings we look for patterns we kind of we want answers to things we see we see kind of constellations of symptoms and we try and put them together and find a solution. Sometimes you will be barking up the wrong tree. But I think again it comes back to listening to that patient’s perspective trying to understand why they feel that that diagnosis is appropriate to them and then seeing if they meet the criteria to meet their diagnosis or if or if maybe there’s something else going on that needs to be explored. It comes back to that thing of understanding each other’s processes, each other’s priorities and just being open-minded to the fact that you both do want to help. It sounds like your experience wasn’t particularly fruitful but, in general, if you both bear with each other and try to understand each other’s motivations then you will reach a conclusion and it may not be where either of you thought you’d end up but it may be the right place when you get there eventually.What does a doctor think about seeking a diagnosis for a chronic condition?
Jesse. I suppose that’s one of those tricky parts is that I think there is still this situation in society where doctors are revered and you kind of assume that they can like give you an answer within a single meeting. It’s important to remember that doctors are human beings and they’re prone to getting things wrong or needing time to figure things out. Especially if the [conditions you go to them with] are harder to diagnose. I think it was certainly part of my experience too as I had this expectation that I would just be given a diagnosis and maybe that didn’t help with that process either where I was adamant that that’s what was going to happen and so my reaction when that didn’t happen was to be maybe very dismissive. I guess the natural follow-up question is; being aware that you know a diagnosis can take time and that you need to be patient, that you need to present your case over a period of time. What are the steps that a person who is seeking diagnosis should take? Should they be trying to figure out if their doctor, their current GP, is the right doctor for them to be talking to? Should they switch doctors? Can they present health journaling or health-tracking or some sort of data to show – in my example – dramatic weight loss a food diary that shows that I haven’t necessarily been eating everything I should be? What are the steps you’d recommend for somebody who’s doing that [experience seeking diagnosis for a chronic condition] for the first time? Dr Johannes. So, first of all, I don’t think anyone who feels that they have an eating disorder should try and demonstrate dramatic weight loss I don’t want to kind of incentivize anyone to lose more weight to try and hit a diagnostic criterion that’s absolutely not where we want to go. Jesse. Just to clarify. I mean that if I had been journaling my existing weight loss, would that information have been helpful? Dr Johannes. I think, again, it really depends on the doctor you’re talking to and it depends on the patient’s life. if it’s something that you find really helpful I think regardless of what your doctor thinks, I think it’s worth doing because if it gives you an understanding of what constitutes a good day or a bad day and what other things are associated with that. I think that can be a really therapeutic tool to help you manage the day-to-day. It may not be something that’s going to solve the problem or give you a cure but I think it can be therapeutic in helping you to understand the symptoms you’re experiencing and how you’re feeling day-to-day. I think for some doctors they would love it and for some doctors, it will just eat more into that kind of precious ten minutes that you have to try and fix everything in the universe which is always difficult. In terms of changing your GP, again it’s a really – I know I’m saying tricky a lot – it’s really tricky. Because I think if you move [from GP to GP] a lot and your medical record shows that you’ve kind of gotten through six or seven GPs in a year. That’s immediately going to kind of create this impression before someone meets you and no matter how open-minded someone is if someone sees that a patient has moved six or seven times in a year you’re subconsciously going to be wondering what’s going on. A hundred things will go through your [GPs] mind but for most GPs it would make you a little bit wary of what’s going to happen. At the same time, I think absolutely! If you meet with your GP for the first time and they’re dismissive of you and they don’t listen to you and they try to pigeonhole you in a certain way and you just feel that that relationship is never going to go anywhere. Then absolutely, the right thing to do is to try someone else. You could just ask to see someone else from the same practice if you’re at a practice with more than one GP, which is most of them these days. I think again it’s about taking time, having realistic expectations about what can be achieved, you know? Everyone has bad days, GPs have plenty of bad days so it might be that you just caught someone on the wrong day and they’re rushed off their feet, it’s late in the day, stressed, whatever else. And I wouldn’t dismiss an interaction on the first go. I know that’s really difficult because a lot of the time you’ll wait weeks and weeks and weeks for an appointment and then if you have an unsatisfying interaction with someone you feel like that’s a month that’s gone down the drain because that was your one opportunity to advocate for yourself. That’s frustrating for the patient but it’s frustrating for the doctor as well, because as I keep saying – in general – we want to help and it’s really frustrating when we have an unsatisfactory interaction with someone. So I think you know if “this person is never going to understand me” then maybe speak to someone else in the practice. Maybe speaking to someone other than a doctor in the first instance would be useful [too]. So I don’t know if you know about social prescribers but sometimes they’re a really good point of contact in a practice. Not everywhere has a social prescriber in-house but they’re just incredible people who can fix things in your life which doctors don’t know about but have traditionally sometimes ended up doing. So anything to do with housing or lifestyle issues, finances, all of those kinds of complicated life skills that you’re just expected to have as an adult; Social prescribers can often help with. Sometimes as a kind of interim measure as something that runs in parallel [to diagnosis and treatment], they can be really good people to help you get other parts of life under control and quite often they’ll have access to some of the services that a doctor could refer to as well. So, I think yeah, look at other GPs in the practice if you’re struggling. Look at other people in the practice in general who might be able to give you some initial support. And it’s a two-way relationship where you both have to build trust with each other. You have to understand each other’s pressures and points of view and – I think – if you can see that a GP or another doctor is someone that you could potentially build a kind of understanding with, then just be prepared for that to take a little bit of time and it will get there. There will be frustrating times but that’s just part of the human experience.Should you take someone with you to a doctors appointment?
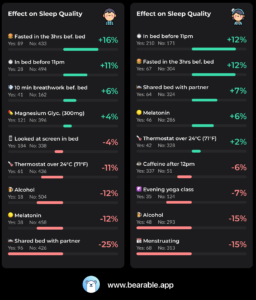
Jesse. I suppose that if you have a hard to diagnose condition, it’s going to be hard to diagnose for any GP, right? So I think it’s maybe accepting that it could take a bit of time before that happens and finding a person [a GP] that you feel will hear you, and will work with you in a way that you feel comfortable with [is what’s important]. Maybe treating it more as a typical human interaction, where – rather than having set expectations about what a doctor should be doing – actually talking to them and saying “what do you need from me” and “how can I help you to understand what I’m living with”. Kind of along those lines, I suppose often it is – or it can be – difficult to explain your symptoms to a doctor especially when you know there’s a small window in a window of time that you have to do that. I know that as a person with depression and anxiety; brain fog and memory loss, as well as having quite a wide array of symptoms can make it hard to explain exactly what’s happened in the last few months of my life. That have made me feel like I want a specific diagnosis. In the past you’ve mentioned taking somebody with you to advocate for you [at an appointment with a Doctor]. Is that something you want to talk about a little bit as well? Dr Johannes. Yeah. I think it’s a good insurance policy because if you have been waiting a month to get an appointment and you’ve got 10 minutes to make your case, that’s a really high stakes situation to be in. That extra stress can make you struggle even more to kind of fully make use of that time efficiently. So I’ve had a lot of patients come in before, they’ve just written everything out that they’re experiencing. And, although that can sometimes be overwhelming because it might be a list of ten different things and we have to pick one or two of them. That can be one way just to remind yourself. As you said, I think if you talk through a situation with a friend before you go to the GP that can be really helpful for a number of reasons. First of all, I think to have another person’s perspective – and someone that you already trust to give you their perspective – and to help you just organize those thoughts and pick out what’s really important. Then to be with you to just give you a bit of confidence, to maybe steer you in the right direction if you do go off track, and to make sure you get those key points across. I think that can be really helpful. Obviously in the time of pandemics – and all kinds of other chaos – it may not be feasible and even if it’s a telephone conversation [with your GP]. Having someone around is a good idea. I think in general, most GPs would be on board with that. I think also if someone comes in with a kind of an advocate or a friend, as long as you know they’re happy with confidentiality, and with having information shared with them. I think that can be quite reassuring for the doctor as well. Because, as I said, I think you know we want that interaction to be efficient and smooth and we want it to be high yield as well. We want to be able to get as much done as possible in that brief interaction. So [if] there’s someone there who’s helping to steer us back onto the right track and maybe to just almost kind of mitigate some of the possible tension. Because they’re removed from the situation – to some extent – they may be better placed to kind of understand both the doctor’s stress and the patient’s situation. I think it’s pretty much a win-win. At the moment you know that might be that might need to be a friend on speakerphone while you’re having a consultation with a GP. I think it’s just a good idea. The other thing you’ve mentioned to me before is having a record of your symptoms or looking at kind of correlations between things [related to your health]. Again I think for some GPs that will work really well. I think the problem we sometimes have is that we have kind of very specific ways of giving someone a diagnosis or looking at the severity of depression or anxiety or something. So we have our own tools and they are quite intuitive, they’re not difficult to apply but I think they’re kind of less useful for someone with those symptoms to use in their own time. I think apps like Bearable can be really good for people to get a better understanding of what’s going on and what triggers and what symptoms will lead to a better day rather than a worse day. I think offering those [types of information] to your GP is worth a go and – you know – it’ll either work or it won’t work but I think it goes back to being open-minded [and] giving everything a shot. Accepting that some things won’t work. Accepting that you know everything’s personal. Everyone has their own preferences. But it comes back to treating your doctor a bit more like a human being and “saying is this something that you would find useful” and offering it as an option rather than assuming that having – potentially an overwhelming amount of Data – could only be a positive thing. [Understanding that] it could be something that actually hinders the process too [for some GPs] I don’t want people to feel like I’m just saying that “you need to treat your doctors better”. I’m just saying that everyone just needs to appreciate that this is complicated stuff and it will take time. Doctors need to be a lot more empathetic towards patients as well. It’s a two-way street.What do doctors think of self-diagnosis?
Jesse. I think that’s a really positive thing to hear because – often – for people with chronic illnesses or hard to diagnose illnesses there are a lot of negative experiences with doctors. I think it’s right to want to share the experience from the other side as well. To hear that it can be hard for a doctor to fully trust and understand or to meet the expectations of a person who has self-diagnosed. I think a lot of that frustration comes – on the patient’s side – from the fact that it can be hard to treat something if it’s not being diagnosed. So I think you often see that people within these communities of – whether it’s chronic conditions or hidden illnesses – there is a lot of self-diagnosis. Just because there’s a degree to which it’s validating to say “okay I belong to a community of people”. [A community] who can say that there are these certain solutions, whether it’s alternative treatments or something else, that can help. Because ultimately a person wants a diagnosis so they can begin to manage and treat their condition. Do you have any thoughts about the benefits or limitations of self-diagnosis? [And can you also touch on] how a person who’s struggling to get a diagnosis should try and treat something that they feel that they have? Dr Johannes. Will you forgive me if I say it’s tricky? Just addressing one of the earlier things you said I think that the idea of a diagnosis giving you access to a community of people with similar experiences. I think having a doctor tell you that you have something shouldn’t be … the doctor isn’t the gatekeeper to you having access to that community. I think if you have a collection of symptoms or a collection of experiences that make you feel like you belong to that community, then you belong to that community. That’s not for me [as a doctor] to say. I’m certainly not going to police your interaction with that community. So, I would totally encourage people to engage with communities of people who share some of their symptoms and experiences. I know that you and I have looked at one instagram page, for example, where they just look at all kinds of complicated medically unexplained symptoms. Just less common conditions which are maybe not adequately managed. It just brings people together to discuss what works for them and I think that’s really helpful. It also raises the point that we [Doctors] may be able to give you a diagnosis but it doesn’t mean that we’re able to suddenly give you a treatment that’s going to be incredible. I think it’s like you were saying there’s this expectation that doctors have access to treatments that just work and quite a lot of the time that the most effective treatments might not be something that comes from a doctor. I think one of the really typical and distressing things for the medical profession can be when – in the case for example of chronic abdominal pain – when we have patients who end up undergoing regular exploratory abdominal surgery. Having operations to look into the pelvis and into the bowel to see if there’s something wrong. Because a patient presents with such excruciating pain or difficult symptoms and it comes to a point where we have to surgically explore that abdomen. And – you know – sometimes you find something and sometimes we have to explore a bunch of times before you find that actually there is endometriosis there (or something else) BUT there’s a huge number of cases where a patient will have operation after operation after operation and there’s nothing there. That’s just a situation when the answer to those problems isn’t surgical and it may not be medical. I think the more you can engage with communities of people who have similar experiences the more you can find other ways to manage these conditions. Sometimes even the best medical treatment – for example with chronic pain – there are lots of medications you can take. You can escalate medication up to a certain point but at the end of the day, with some chronic pain, the ultimate and the most important part of that strategy is learning to cope with it. Accepting to some extent that you know – “I’m having real physical pain and no amount of medication is going to fix that” – and I can either live a life where I’m experiencing really intense side effects from all the medication I’m taking and my quality of life is poor. OR I can learn, to some extent, to cope with a certain level of pain and have really bad days and some okay days. That’s obviously not an ideal situation; it’s not something that anyone would wish for. But again it’s about managing expectations and having people listen to you and sometimes the doctor isn’t the right person to listen to you because it’s not something that we have the resources to do. If we could sit there with every patient for half an hour or more and just kind of help them to get through this stuff I think a lot of people would love to do that. But it’s just not the situation that we live in. It’s not the system that we live in. So I think sometimes it’s just the wrong place to go looking for it. I think finding a really strong community of people with similar experiences can be really useful. I would say the counterpoint to that is that I think if you find you’re in a situation where a group of people are trying to find ways to get around the medical system to kind of subvert it to get into treatment, or to get a diagnosis, or if it becomes kind of adversarial. Where it becomes a melting pot of ideas about why medical professionals are bad. I think that’s obviously not going to be as fruitful. But if it’s a positive sharing of experiences and you know and anecdotal knowledge from people about what’s helpful. I think that can only be a good thing.What do doctors think about alternative and holistic treatments?
Jesse. I think one of the benefits of communities may be that it opens people’s minds to the fact there might not be a single treatment that works. I think you’ve talked in the past about how symptoms can be on a spectrum and I think my experience with having met a lot of people with different hard to diagnose illnesses or chronic conditions is that they can be very unique to each individual. A medication or a holistic treatment that works for one person isn’t necessarily going to work for everybody [with that condition]. Do you think in the same way as having an open mind about diagnosis it’s maybe important to have an open mind about the types of treatment that might work for you as well? Dr Johannes. Absolutely I mean every situation, every patient is really different and one of our jobs is doctors are to try and simplify everything and you know put everyone in a box with a specific treatment plan. Because that makes it manageable and bearable. So, yeah I think being open-minded to the treatments as well is really important. I think most doctors, in general, would advocate for people exploring kind of safe alternative therapies alongside any recommended medical therapies. I think what is recognized is that the major benefit that people get from alternative practitioners – regardless of what their approach Is – is that they do have that time. They have time to empathize. To a great extent, they have time to listen and they use physical touch in a way that’s very therapeutic [and] which is either inappropriate or out of context in a medical consultation. If you have massage and acupuncture the needles themselves may have little or no effect – from a purely scientific standpoint – but the fact that someone has physically interacted with you, showing you that they care, and provided a service to you which you felt would help you without asking questions. I think that has huge therapeutic benefit and I think one of the things that we struggle with in general, as a community, is the idea that a placebo can be a good thing. It’s not being disparaging if I said that I thought that acupuncture was largely a placebo. If it has a positive effect for someone who’s really struggling to get help and they find that it alleviates their symptoms that’s an incredibly positive thing. An incredibly good thing. I think the tricky thing then is you know if it’s that effective why isn’t it available on the National Health Service [NHS] and then we get into a whole discussion about how clinical trials testing is against a placebo. So the placebo effect is discounted in those situations and it becomes difficult to justify an expensive placebo as opposed to a cheap one. But that’s a whole other shebang. Jesse. Yeah, I don’t know that we should get into that conversation right now because I think it’s quite a big one. Ultimately what you’re saying is that it could be important for people with any kind of diagnosis to be open-minded and to try different treatments. Whether they’re medically prescribed or not, if they have a positive impact for you then that’s only a good thing. Essentially a medical diagnosis and a medical treatment might not be the only solutions for a person. Dr Johannes. I would say that I think it’s worth telling your GP what other things you’re trying. Not necessarily to get their opinion on it, or to try and get it on the NHS – or even to say that you don’t want to engage with the GP anymore because something else is working – BUT I think – particularly with alternative herbal supplements for example – there are some which have really significant interactions with other medications. So I think it’s important to kind of keep your GP informed of what other things you’re trying. And I think if you find something that’s really working your GP will be really happy to hear that you found something that is helpful. I like to think of them as complementary therapies rather than alternative therapies because hopefully, you’ll have a GP that understands that if something’s helping you that’s a good thing for everyone. Jesse. Are there any alternative therapies that are offered through the NHS that we can talk about? Dr Johannes. There are. I think the funding is very different in different areas and so different things will be commissioned by different services and by different groups within the NHS. So there isn’t a kind of straightforward answer to that but I think certainly in the past there were some areas that would offer acupuncture or dry needling for certain conditions. But again because it’s on the NHS there are quite specific criteria about who would be eligible for that so it’s something you can discuss with GP. I think they’re becoming less common rather than more common but certainly, if you have an open discussion with your GP they’re going to be honest with you about what’s available. Equally, if you’re someone who has chronic pain you’re being managed by a pain team in the hospital they’ll know what’s available in your area. So again it’s kind of a case of asking and finding out rather than having its own assumptions about what might be available.How can someone manage the experience of seeking a diagnosis for a chronic condition?
Jesse. Ultimately what I think we’ve talked about today is that it’s tricky from both sides, right? That’s the word you’ve used repeatedly. I think assuming that it’s not going to be a quick and easy process [to get diagnosed and treated], acknowledging that this is something that takes time, probably takes a number of conversations, and it involves some form of relationship building with your GP. That’s obviously difficult in itself if a person has chronic pain, chronic fatigue, or depression. Is there anything that can kind of help a person to manage that experience? I think you’ve touched on things like CBT in the past that can maybe help to give somebody some techniques or some ways to manage – even just that experience [of obtaining a diagnosis and treatment] – even if it’s not going to help them with their symptoms or their overall condition. Dr Johannes. There are a few things [to unpack] there but yeah – in general – I think CBT is a really good approach. I think if cbt was something that was just part of a curriculum that we all went through when we were younger I think the world would probably be a better place. Because essentially all it is it’s a set of tools that help you reframe your experiences and reframe just your day-to-day life in a way that makes it make a bit more sense and makes it more manageable. I think that one of the problems we have is that when we suggest cbt it immediately kind of takes the conversation down the “Are you saying it’s all in my head? Are you calling me crazy? Are you trying to make this a mental health diagnosis as opposed to physical health diagnosis?” path, and I think that’s a kind of real branding nightmare for CBT. That it’s seen as something dismissive rather than being seen as a really kind of concrete proactive step which we could probably all benefit from. So I definitely think that’s something worth doing. It’s something that you can just teach yourself online or from books or from audiobooks. So I think that’s something that’s worth having a look at. Obviously, if you access that kind of service through the health service then there can be massive delays involved just because it’s such a demand of service and then the quality of the CBT you get might not be perfect quality. I would still recommend people embrace it if they’re offered it through their doctor. But equally, if you’re someone who’s kind of motivated and is able to invest the energy [into it] – because I know a lot of people just won’t be able to bring themselves to pick up a book and plough through it – I know that can be a really difficult first step. But if you can, I would encourage you to give it a shot. It certainly can’t do any harm and I think it can help a lot of people. The other thing – as we’ve said – is that there’s a lot of bad press around the way people perceive a mental health diagnosis vs. a physical health diagnosis. I think that’s a real problem with modern medicine is that we really distinguish between those two things. We have to see them as intertwined in the same way that we’re increasingly recognizing that you know the gut and the brain are kind of intimately interconnected. Having gut symptoms can be a real physical manifestation of things happening in your brain or in your mind. We also need to accept that all of your physical symptoms are to some extent a reflection of what’s happening in your mind and in your brain. Your brain has the power to massively amplify or massively silence symptoms like pain. Also physical things like what we would call a pseudoseizure or other kind of real physical visible manifestations and symptoms can be something which your mind and your brain are creating. It’s not to say that they’re to do with being crazy or having a pure psychiatric problem. But that the mind and the body are so intertwined that you have to accept that for any condition there’s going to be some psychology and some psychiatry kind of interwoven into that. Again it’s part of embracing a really kind of broad approach to treating people. You need to have a really holistic view. This is maybe ironic coming from a doctor because that’s probably what patients have been telling us since the beginning of time. But I think when a treatment is offered you have to weigh up 1. could this potentially help me and 2. In the worst-case could it do me any harm? I think if you’re offered psychological treatment I can’t imagine that there is any potential harm. So I think even if you, even if your instinct is to kind of turn your back on that and say that sounds dismissive, I want to avoid that, just try it. What’s the worst that could happen? Someone is offering you something to try to help even if it may not be the thing that you primarily want and even if you think it might not be the most beneficial treatment for you. If it’s going to improve your symptoms by five per cent then carpe diem. Jesse. I suppose that if it doesn’t work for you, you can check it off and say “Well I tried that, what’s next? What else can I try?”. Which helps you get closer to finding the treatment that works best for you. Dr Johannes. I think the caveat is that some things you need to try for a period of time before you decide that they haven’t worked for you. And you know there are lots of medical therapies where you have to wait a couple of months before you know if there’s a benefit. There may be – for example with SSRI, a type of antidepressant which is commonly used – your symptoms in the first couple of weeks can be much worse. So there can be a really difficult time where you have to just cope with the rough patch to get to the smooth. But yeah I think you’re right. That it’s worth trying things in general and if they absolutely don’t work or they haven’t helped then yeah cross them off the list. Just say “thank you for offering me something, it didn’t work. What’s next? Let’s move on!”.Is there a cure for your chronic condition?
Jesse. I suppose, with that, is again acknowledging the idea that there might not be this perfect panacea cure-all and that things will take time and then it might be useful to have coping mechanisms and things in place to help you with that process as well. Rather than thinking “I have a chronic condition that I can cure” it’s more about thinking “I need to go on this journey of finding all the things that can help to manage this”. Is that something that’s represented in a way that a doctor would approach it too? Are you presenting treatments as solutions or are you presenting them as things that may or may not help? Dr Johannes. I think yeah it’s a really interesting question. I think medicine, in general, is becoming more kind of protocolized and – like I said earlier – we have a tendency to kind of recognize a pattern, slap a label on something, and then push it into a protocol or an algorithm that says that “if this and this is the case, then you refer to this service”. Then they’ll have an algorithm for what they do next. So I think in that respect then to some extent yes we do kind of say “congratulations this is your label, this is the pathway that you go down” and the intention is to make you feel better. I think in general doctors do try and avoid promising a cure where the chance of having a cure is low. I think doctors are getting better at establishing reasonable expectations but it’s really varied. Different people will have a different skill set and you may get some doctors who are just less experienced in this area and they do give false expectations or kind of give people the impression “yes I’m going to give you this label and in a year because you’ll be better”. Jesse. It lends itself to having conversations with your GP and understanding their approach to your situation. Then determining if they’re the right GP for you before continuing that conversation. Then at that point, you might choose to go somewhere else and find somebody that maybe has more expertise or a more sympathetic view of your condition. Dr Johannes. One of the GP practices I worked in recently. There was a really stark difference. There were a couple of GPs who are very much business-minded like “crack through the patients! Solve the problems as quickly as possible!” and they would find it quite frustrating if there was a complex situation that came up. Then there were another half of the practice who were very empathetic and they would spend a long time with their patients and they’d end up staying late a lot because they were kind of going in-depth [with everyone]. I think as a patient, I want that “wham-bam in-and-out” you know? Get your prescription and go!” I would find it really frustrating if I was being seen by a GP who is really trying to kind of connect with me on a deeper level and explore things. It’s certainly not saying that there are good and bad GPs but it’s like the Tinder of medicine; you have to kind of keep swiping until you find a personality that matches with you. You may find that they are in the same practice. Equally, there are a lot of times when in a 10-minute consultation we really struggle to kind of get to the bottom of something and we need to go away and discuss it with all of our colleagues. Quite often we’ll have a clinical meeting a couple of times a week where we discuss things that we can’t quite get our heads around. Then after having a conversation with a bunch of different people with different levels of experience and different approaches. Then it may be that the next consultation you have with your GP is just much more rewarding for both of you because in that interim period they’ve gathered insights from other people that they can bring to the table. I would never [make a decision about a GP] on a single encounter with and then snap away from it. Obviously, there are situations when that would be appropriate. But I think in general; give things a chance and just see if you can make it work.Are there resources that can help people who are seeking a diagnosis for a chronic condition?
Jesse. I think that’s the most useful piece of advice from this conversation. Just trying to build a relationship [with your GP] and be patient with that experience so you can get the most out of it rather than making snap judgments based on maybe not being instantly diagnosed with something that’s difficult to diagnose in the first place. I think we’ve been talking for a little while and I don’t necessarily want this to run on too long. I think there’s probably a few other things we could talk about but for now, do you maybe want to talk about any resources you want to recommend or anything else you want to touch on before we kind of wrap things up? Dr Johannes. Yes I think you mentioned that we’d probably kind of leave a list of links somewhere afterwards anyway I think just having a look at what was available myself just from a cheeky search on the internet earlier. It’s interesting to see if you go through the NHS website it has a pretty good summary of how I think how most GPs would approach what we call “medically unexplained symptoms” which can range from things like chronic fatigue syndrome to IBS, fibromyalgia, etc. Which I think are some of the common things that the GPs see within this category. I think it’s a quite reasonable review of the kind of things we’ve talked about. It talks about CBT, it talks about some medication, and it talks about if you think that your GP has missed something. It talks about things you can do from a self-help perspective as well. Then one of the other resources that I came across was the national organization for rare disorders which I think it’s a UK organization because it talks about the collaboration with some trusts in London for example. That frames it [chronic conditions] in a very kind of neurologically focused way as opposed to things being more psychological. And I think all of you know when you go on this journey of trying to find ways to manage your condition and manage your symptoms and your experiences. I think part of it is just about finding voices that reflect how you see your world. So I think it’s really interesting to see that there are resources that kind of view things in a kind of quite primary care, relatively holistic way and there are other organizations which kind of talk about it from a very neurological point of view. I think for some people that would be really helpful just because it may be the way that they understand their experiences. That may empower them in their own way. The third and final one that I came across was a website called patientvoices.org.uk which looks at stories from patients, carers and from members of the staff as well. I think just in terms of becoming someone who’s more self-aware and more aware of the experiences of people around them and communities of people that have similar experiences. I think it can be really really useful to see those stories, to read those stories. Because I think sometimes your closest friends and family might have had those conversations with you, but I think if you hear those stories from people who are slightly removed from your situation you can get some different perspectives on what you’re going through. I think that can be really therapeutic.Should you learn the medical terms for your chronic condition?
Jesse. I think it’s one of the things we hear very often especially in the kind of hidden illness world is “you don’t look sick” and that can be something that friends or family might say to you because you maybe don’t have these like visible symptoms. I’ve definitely seen huge communities on Reddit of people with very very niche chronic conditions who essentially exist to provide advice and support and validation and recommendations. Because I think it can be quite lonely if you have something that you’re not able to diagnose. You can’t say “I have evidence that I have this thing” or “a doctor has confirmed it”. So it can be a bit alienating. I think finding communities and other people who have similar experiences is quite an important part of this process. To touch on the second resource you recommended as well, I wanted to ask if it’s useful for somebody seeking a diagnosis to have some of the medical vernacular or some of the like medical terms for what they’re dealing with? So they can speak about it in a more medical way versus maybe referring to things maybe in a more generic or non-medical way. Dr Johannes. Is it useful for a patient to come to you and say like here are the specific things I’m experiencing based on the research I’ve done? I think that’s such a difficult question because I think sometimes when someone comes into a consultation and they’re kind of equipped with a certain level of kind of medical language or a degree of medical insight it can again sometimes just throw the consultation off because it’s not something that we’re prepared to hear. I mean some GPs will find it really useful but sometimes it throws that relationship off a little bit. I think it’s completely worth reading up about the symptoms you’re experiencing and the diagnosis that you think might be relevant to you. But I think being authentic in that consultation and just talking through your experience of symptoms just from how you actually experience them rather than trying to pigeonhole yourself into specific medical language I think can be much more rewarding. Because if a doctor has seen similar patients with similar experiences and symptoms before that’s much more likely to trigger something in our minds that says oh this reminds me of the patient I had which has this kind of unusual set of symptoms I had to refer on to this person. But if you have someone who walks in and starts talking in medical language to you, it may just not trigger that same light bulb, or it may seem that the patient has some kind of weird agenda. Maybe we [the GP] then go off on a tangent trying to explore that slightly mysterious agenda which may just be the patient wanting to be more efficient and it ends up kind of making things take a weird turn. So I think; educate yourself about your symptoms and about things that you think are maybe going on. But I don’t think you should try and translate your experiences into medical language just for the purpose of trying to convey the message to the GP. Jesse. That makes sense. It’s interesting that that could actually throw a GP off and actually take them down a different route as well because it’s a piece of advice I’ve heard a few times from people. I’ve always wondered if it’s actually beneficial or not. I think as we’ve touched on, the most useful thing to take away from this is maybe to have tempered expectations about what to expect from a single interaction with your GP and to approach it as a situation where you need to explore what’s happening together. So that GP can be informed well enough to help you to understand what’s happening. And so they can start to recommend treatments and begin to explore how you manage a condition. Rather than it being a single interaction where you get a diagnosis and a treatment and then everything’s resolved. Dr Johannes. Yeah and the other thing I would like to say is just that brains are incredible and we have so little understanding of how incredible they are. And if your brain decides for whatever reason that you’re going to have symptoms which look like a specific condition, you’ll have those symptoms. And I think one thing that’s really really hard to come to terms with is that if we have done our best to investigate you and diagnose you and we’ve sent you to all of those clinics. There is [still] a chance that – at the end of the day – an incredibly experienced consultant in neurology might turn around to you and say “I’m sorry you don’t have this condition”. I think that can be incredibly devastating for someone who’s spent – probably years – first of all coming to terms with the symptoms and finding the confidence to kind of discuss it with other people and with their doctor. They wait for all of those referrals, and then to be kind of essentially turned down at the last hurdle. I don’t think any of us give enough credit to how incredibly complex brains are and what they can do. There are a lot of people who go through really traumatic experiences when they’re younger – or which are ongoing – and the brain will convert those experiences into physical symptoms. It’s not to say that the symptoms aren’t happening, they will be things that as a doctor I could watch happening in front of me. It’s not that a patient is doing it deliberately or has any control over it. But your brain can make all of those things happen. And I think if you just bear in mind, if you’re willing to accept that, after everything that happens, there’s a possibility that your symptoms might be coming from your brain or from your mind. And as a consequence of something that we can’t define. I think as long as you have that in the back of your mind then it’s going to be less devastating if that ends up being the reason for what you’re going through. It’s kind of a weird way to end things.What to do when a doctor disagrees with your self-diagnosis?
Jesse. I think it’s relevant and it helps to set an expectation that there might not be a diagnosis at the end of this journey. Which I think a certain percentage of the people watching this will find. I think that it’s not an uncommon thing. People do struggle to get a diagnosis. What would actually happen in that situation if somebody determines you don’t have these physical symptoms and it might be something that’s created in your brain? Presumably, there are still treatments and things that can help with that or that might help a person to explore those past traumas or whatever else as well, right? Just because they don’t have the diagnosis they were expecting that doesn’t mean it’s the end of the journey. Dr Johannes. Yeah completely. It’s definitely not the end of the journey and I think that’s why it’s so useful to kind of explore things in parallel as well. So as a medical student many moons ago I have sat in neurology clinics in a hospital where people have all of the symptoms that as a medical student I could think of that would represent multiple sclerosis for example – and you know an incredibly talented neurologist has assessed this and determined that actually, they don’t have MS. Their brain is creating all of these physical symptoms but it’s not because of MS. If that happens, as you say, it’s not the end of the journey it just means that you have to kind of turn 90 degrees and see what happens next. And I think that that’s an incredibly difficult thing to go through. I think there’ll be a grieving process associated with not having a diagnosis that you’ve been working towards for so long. I think it’s important more than ever at that stage to not turn your back on the medical profession, because it [probably] feels like you’ve been rejected by medicine. Essentially it’s just another thing you’ve crossed out on a really really long to-do list and it just means that there’s going to be another period of reflecting on your experiences reflecting on your symptoms and it’s not going back to square one because you’ve you have made progress through all of those years of working on reaching that stage. It feels like a massive setback but at that stage, just try not to feel rejected and try to – you will you’ll grieve you’ll reflect a lot but at some point – come back to medical practice and say “I’m willing to consider that maybe that was the wrong diagnosis, where do we go next?”. It’s about finding a way to be strong enough to take your GP with you on that journey. Not to see them as having you know booted you out of the system and said “you’re faking it” or “we don’t believe you” because that’s not at all what is happening. Jesse. I guess a positive way to look at that really is the sooner a person begins this journey and finds the GP who they can have a conversation with and who will explore this with them. The sooner they can start working towards that path and either obtain the diagnosis they think they should have or even having that diagnosis ruled out. Then looking at what other courses [of action] there might be as well. So I think maybe that’s a positive way to look at that as well. Just to go and have those conversations to begin with so you can start heading down that path. Rather than putting it off because of past negative experiences with GPs, or having the wrong expectations about what might happen in an initial consultation. Well, thank you for talking about everything today. I think it’s been really interesting. I think if I’d had access to some of this information or these perspectives it would have helped me 10 years ago when I was first seeking a diagnosis. So I hope that these bits of advice are useful for people listening as well.Resources mentioned in this episode.
Photo credit.
Photo by Karolina Grabowska from Pexels